Fill in a Valid Medication Administration Record Sheet Template
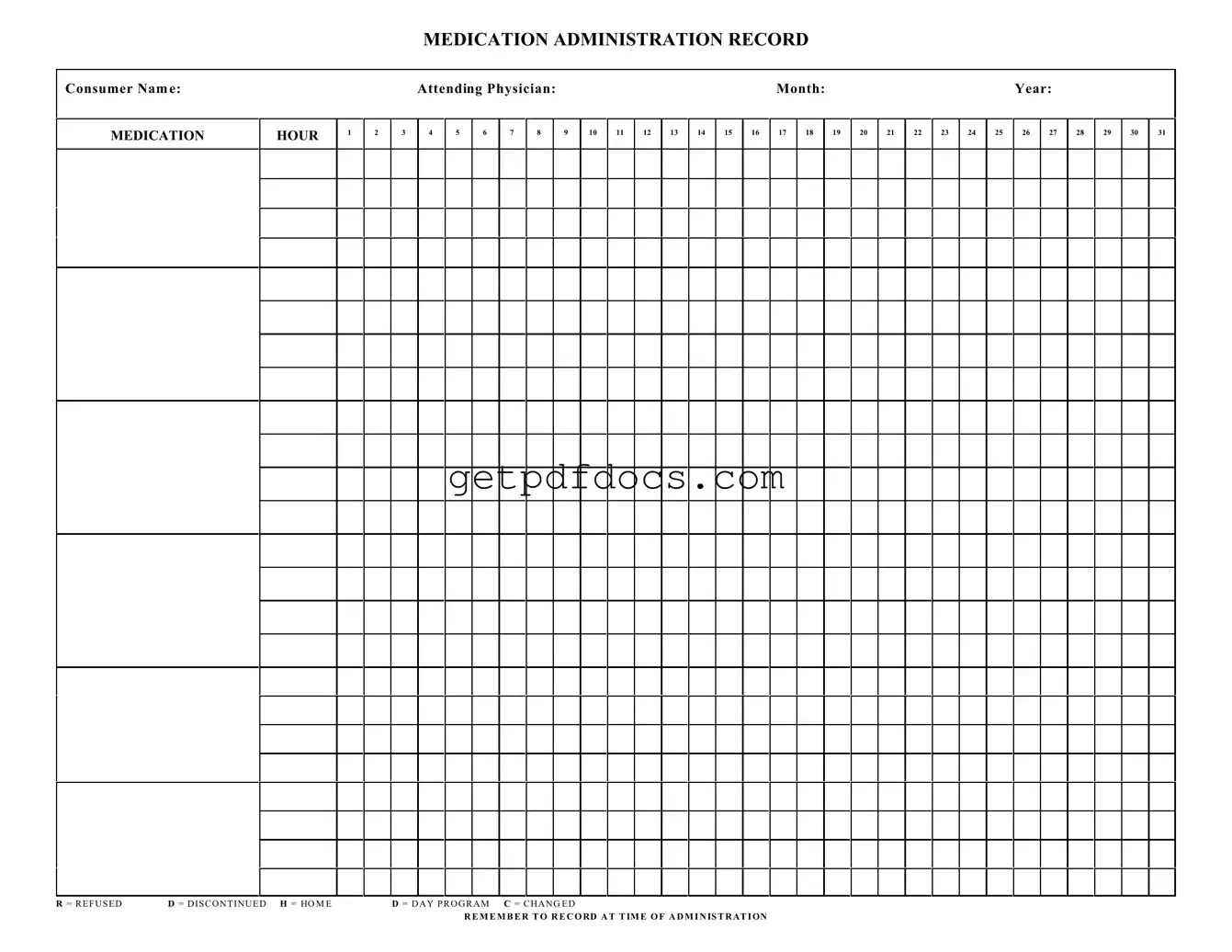
The Medication Administration Record Sheet is a vital tool used in healthcare settings to ensure that patients receive their prescribed medications accurately and on time. This form includes essential information such as the consumer's name, the attending physician, and the specific month and year for tracking purposes. It features designated hours for medication administration, allowing healthcare providers to document when each dose is given. The form also includes various notations, such as 'R' for refused, 'D' for discontinued, 'H' for home, 'D' for day program, and 'C' for changed, which help in maintaining clear communication regarding any changes in the patient’s medication regimen. It is crucial for staff to remember to record the time of administration, ensuring that all medication details are accurately captured. By utilizing this form, healthcare providers can enhance patient safety and improve overall medication management.
How to Use Medication Administration Record Sheet
Filling out the Medication Administration Record Sheet is essential for tracking medication given to a consumer. Accurate documentation ensures that all medications are administered correctly and helps maintain a clear record for healthcare providers.
- Begin by entering the Consumer Name at the top of the form.
- Next, fill in the Attending Physician name.
- Indicate the Month and Year in the designated fields.
- For each medication administered, locate the corresponding hour in the row labeled MEDICATION HOUR.
- Record the date of administration in the appropriate box for each day of the month.
- If a medication was refused, write R in the box for that day.
- If a medication was discontinued, write D in the box for that day.
- For medications given at home, mark H in the appropriate box.
- Indicate D for medications given during a day program.
- If there was a change in medication, write C in the box for that day.
- Remember to record the time of administration in the designated area.
Key takeaways
When using the Medication Administration Record Sheet form, it is essential to follow specific guidelines to ensure accuracy and compliance. The following key takeaways will help you effectively fill out and utilize this form:
- Consumer Name: Always include the full name of the consumer at the top of the form to avoid any confusion.
- Attending Physician: Record the name of the attending physician to maintain clear communication regarding the consumer's medication.
- Month and Year: Specify the month and year for the record to ensure proper tracking of medication administration.
- Medication Hours: Use the designated hours (1-24) to document when each medication is administered.
- Refusal and Discontinuation: Mark 'R' for refused medications and 'D' for discontinued medications to keep an accurate account of the consumer's treatment.
- Home and Day Program: Indicate 'H' for home and 'D' for day program to clarify the setting of medication administration.
- Changed Medication: Use 'C' to denote any changes in medication, ensuring that all staff are aware of updates.
- Record at Time of Administration: Always document medication administration at the exact time it occurs to maintain an accurate record.
- Daily Tracking: Ensure that each day's medications are recorded daily to avoid gaps in the consumer's treatment plan.
- Review Regularly: Regularly review the completed Medication Administration Record Sheet to ensure all entries are accurate and up to date.
Common mistakes
Filling out a Medication Administration Record Sheet can be straightforward, but many people make common mistakes that can lead to serious issues. One frequent error is not providing the consumer's name clearly. This can create confusion, especially in facilities where multiple individuals receive medication. Always double-check that the name is spelled correctly and is easy to read.
Another mistake involves the attending physician's name. If this information is missing or incorrect, it can complicate communication with healthcare providers. Ensure that the physician's name is accurately recorded to avoid any miscommunication regarding medication administration.
Many people also overlook the importance of documenting the time of administration. Failing to record the exact time can lead to misunderstandings about when medications were given, which may affect the consumer's health. Always remember to note the time immediately after administering the medication.
In addition, some individuals forget to use the correct codes for indicating medication status. Using codes like R (refused), D (discontinued), or H (home) incorrectly can mislead staff and impact the consumer's care. Familiarize yourself with these codes and apply them accurately to maintain clear communication.
Finally, it’s essential to review the entire record for accuracy before submitting it. Errors can slip through the cracks, leading to potential health risks. Taking a moment to double-check the completed form can save time and prevent complications down the line.
Documents used along the form
When managing medication for individuals, several forms and documents work in conjunction with the Medication Administration Record Sheet. Each of these documents plays a critical role in ensuring accurate tracking, compliance, and communication among healthcare providers, patients, and caregivers.
- Medication Order Form: This document provides detailed instructions from a physician regarding prescribed medications. It includes the medication name, dosage, frequency, and any special instructions. This form ensures that caregivers understand exactly what is required for each patient.
- Patient Medication Profile: This profile outlines all medications a patient is currently taking, including over-the-counter drugs and supplements. It helps prevent drug interactions and ensures that all healthcare providers are aware of the patient's complete medication regimen.
- Consent Form: A consent form is essential for obtaining permission from patients or their guardians before administering medication. It serves as a legal document indicating that the patient understands the treatment plan and agrees to it.
- Incident Report: In cases where a medication error occurs, an incident report documents the details of the event. This report is crucial for analyzing what went wrong and implementing changes to prevent future errors.
- Civil Case Cover Sheet (CM-010): This document is essential for initiating a civil case in California, helping courts categorize cases and collect important information. For detailed guidance, refer to California Templates.
- Medication Reconciliation Form: This form is used during transitions of care, such as hospital discharge or transfer to another facility. It ensures that all medications are accurately reviewed and reconciled, preventing omissions or duplications in the medication list.
- Patient Education Materials: These materials provide information about the medications prescribed, including potential side effects and instructions for use. They empower patients to take an active role in their healthcare and promote adherence to medication regimens.
Utilizing these documents alongside the Medication Administration Record Sheet creates a comprehensive approach to medication management. This collaboration enhances patient safety, improves communication, and fosters a higher standard of care.
More PDF Forms
Test Drive Form Pdf - Seek assistance from a salesperson if you have questions during the drive.
For anyone needing to facilitate vehicle transactions while unable to be present, understanding the significance of a Motor Vehicle Power of Attorney is crucial. This document empowers another individual to represent you, ensuring your vehicle-related matters are handled efficiently. Discover more about the process by reviewing this guide on the necessary Motor Vehicle Power of Attorney form requirements.
Dekalb County Water New Service Application - This form allows for quick processing of new water service requests.
Frequently Asked Questions
What is a Medication Administration Record Sheet?
The Medication Administration Record Sheet, often referred to as MAR, is a vital document used in healthcare settings to track the administration of medications to patients. It provides a clear and organized way to record when and how medications are given, ensuring that patients receive the correct dosages at the right times.
Who uses the Medication Administration Record Sheet?
This form is primarily used by healthcare providers, including nurses and caregivers, who are responsible for administering medications. It is also a useful tool for pharmacists and physicians who may need to review a patient's medication history.
What information is included on the MAR?
The MAR typically includes the following information:
- Consumer Name: The name of the patient receiving medication.
- Attending Physician: The name of the doctor overseeing the patient's care.
- Month and Year: The time frame during which the medications are being administered.
- Medication Hours: Designated hours for medication administration, usually listed in a grid format.
- Administration Codes: Symbols indicating if a medication was refused, discontinued, or changed.
How do I record medication administration?
To record medication administration, follow these steps:
- Identify the correct medication and dosage as per the physician’s orders.
- Administer the medication at the scheduled time.
- Mark the appropriate box on the MAR to indicate that the medication was given.
- If the medication was refused or not administered for any reason, use the corresponding code to document this.
What do the codes on the MAR represent?
The MAR includes specific codes to denote various circumstances:
- R: Refused - indicates that the patient refused to take the medication.
- D: Discontinued - signifies that the medication is no longer prescribed.
- H: Home - used when the patient is at home and not in a facility.
- D: Day Program - indicates the patient is participating in a day program.
- C: Changed - shows that there has been a change in the medication regimen.
Why is accurate recording important?
Accurate recording on the MAR is crucial for several reasons. It helps ensure patient safety by preventing medication errors, facilitates communication among healthcare providers, and supports legal documentation in case of disputes. Consistent and precise entries can significantly impact patient outcomes.
What should I do if I make a mistake on the MAR?
If a mistake is made on the MAR, it is essential to correct it promptly. Draw a single line through the incorrect entry and write the correct information next to it. Initial and date the correction to maintain a clear record of changes. Avoid using correction fluid, as it can obscure the original entry.
How often should the MAR be updated?
The MAR should be updated each time a medication is administered. Additionally, it should be reviewed and revised whenever there are changes to the medication regimen, such as new prescriptions or discontinuations. Regular updates help maintain an accurate and current record of the patient's medication history.
Can family members access the MAR?
Access to the MAR is typically restricted to healthcare professionals directly involved in the patient's care. However, family members may be allowed to view the MAR if it is deemed appropriate by the healthcare team. It is essential to respect patient privacy and confidentiality when sharing this information.
Where can I find a Medication Administration Record Sheet?
MAR sheets can often be obtained from healthcare facilities, pharmacies, or online resources. Many organizations provide templates that can be customized to meet specific needs. Always ensure that the version you use complies with relevant regulations and standards in your healthcare setting.