Fill in a Valid Cna Shower Sheets Template
In the realm of resident care, maintaining skin integrity is paramount, and the CNA Shower Sheets form plays a crucial role in this process. This essential document is designed for Certified Nursing Assistants (CNAs) to conduct thorough visual assessments of residents' skin during showering. It emphasizes the importance of identifying and documenting any abnormalities, such as bruising, rashes, or lesions, which could indicate underlying health issues. The form not only allows CNAs to record the exact location and description of any abnormalities but also serves as a communication tool to alert the charge nurse and Director of Nursing (DON) for further evaluation and intervention. Each assessment includes a detailed body chart for precise documentation, ensuring that no detail is overlooked. Additionally, the form addresses the need for toenail care, highlighting the comprehensive nature of resident grooming and health monitoring. By utilizing the CNA Shower Sheets form, healthcare professionals can enhance the quality of care provided to residents, ultimately promoting their well-being and comfort.
How to Use Cna Shower Sheets
Filling out the CNA Shower Sheets form is an important task that ensures proper monitoring of a resident’s skin condition during showering. By accurately documenting any abnormalities, you help maintain the resident's health and ensure that any necessary interventions are taken. Follow the steps below to complete the form effectively.
- Begin by entering the resident's name in the RESIDENT field.
- Write the date of the assessment in the DATE field.
- Conduct a visual assessment of the resident’s skin while giving the shower.
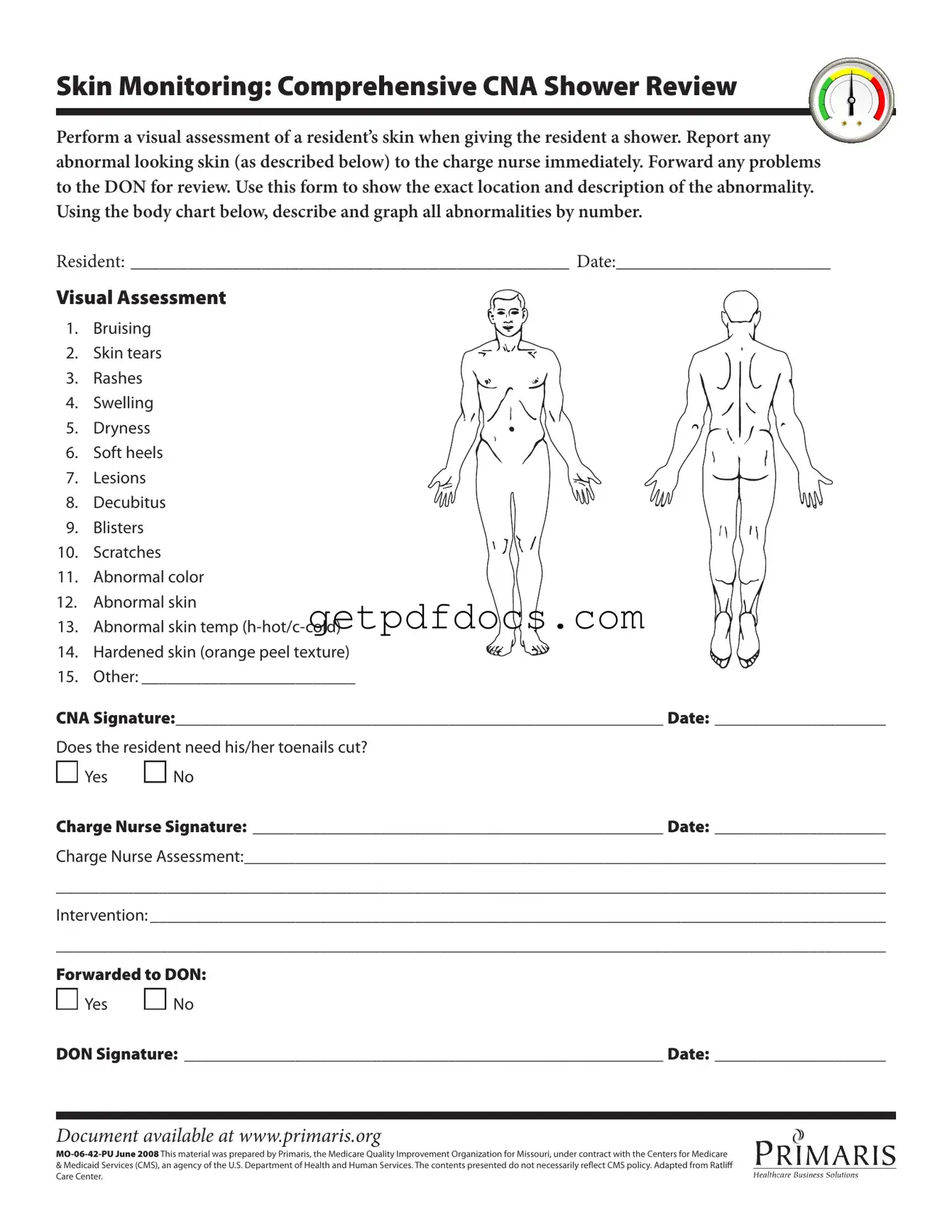
- Identify any abnormalities from the provided list, such as bruising or rashes.
- Use the body chart to mark the exact location of each abnormality by number.
- In the Other field, describe any additional findings not listed.
- Sign your name in the CNA Signature field and enter the date.
- Determine if the resident needs their toenails cut and mark Yes or No.
- Have the charge nurse sign in the Charge Nurse Signature field and enter the date.
- Document the charge nurse’s assessment in the provided space.
- Outline any interventions that were taken in the designated area.
- Indicate whether the issue has been forwarded to the Director of Nursing (DON) by marking Yes or No.
- If applicable, have the DON sign in the DON Signature field and enter the date.
Key takeaways
When using the CNA Shower Sheets form, it is essential to keep several key points in mind to ensure effective documentation and communication regarding resident care.
- Visual Assessment is Crucial: Conduct a thorough visual assessment of the resident’s skin during showering. This helps in identifying any abnormalities that may need immediate attention.
- Report Abnormalities Promptly: Any unusual findings, such as bruises or rashes, should be reported to the charge nurse without delay. This ensures that the resident receives timely care.
- Use the Body Chart: Accurately describe and graph any skin abnormalities on the body chart provided in the form. This visual representation aids in clear communication with the healthcare team.
- Signature Requirements: Ensure that both the CNA and the charge nurse sign the form, indicating that the assessment and any necessary interventions have been acknowledged.
- Follow-Up with the DON: If any issues are identified, they must be forwarded to the Director of Nursing (DON) for further review and action. This step is vital for ongoing resident care.
By adhering to these guidelines, CNAs can enhance the quality of care provided to residents and ensure that all necessary information is documented effectively.
Common mistakes
Filling out the CNA Shower Sheets form is crucial for ensuring that residents receive proper care and monitoring. However, mistakes can easily occur during this process. One common error is failing to conduct a thorough visual assessment of the resident's skin. This step is vital, as it allows the CNA to identify any abnormalities that may require immediate attention. When this assessment is rushed or overlooked, significant issues may go unreported, putting the resident’s health at risk.
Another frequent mistake is neglecting to document the specific location and description of any abnormalities. The form provides a body chart for this purpose, and using it correctly is essential. If a CNA simply notes that there is a rash without indicating where it is located, it can lead to confusion later on. Accurate documentation helps ensure that the charge nurse and other healthcare providers understand the situation clearly.
Some CNAs also forget to check for all potential skin issues listed on the form. This can include bruising, skin tears, rashes, and more. Missing even one item can lead to inadequate care. It’s important for CNAs to familiarize themselves with the entire list and make sure to assess for each condition during the shower.
Additionally, there may be instances where CNAs do not report abnormalities immediately to the charge nurse. This delay can be detrimental. Timely communication is key in healthcare settings, and any findings should be shared right away to ensure prompt action is taken.
Another common oversight is not signing and dating the form correctly. This may seem minor, but it is essential for maintaining accurate records. A missing signature or date can create confusion about who conducted the assessment and when it took place, which can complicate follow-up care.
Some CNAs may also overlook the question about whether the resident needs their toenails cut. This detail is important for overall hygiene and comfort. Forgetting to address this can lead to discomfort for the resident and potential complications if toenails become ingrown.
Moreover, CNAs sometimes fail to provide a clear intervention plan on the form. Simply noting that there is an issue without suggesting a course of action does not help the charge nurse or the Director of Nursing (DON) in making informed decisions. Clear communication about what steps should be taken is essential for effective care.
Finally, CNAs might forget to forward the completed form to the DON. This step is crucial for ensuring that all issues are reviewed and addressed at a higher level. Neglecting to do so can result in important information being lost and unresolved concerns lingering in the care process.
Documents used along the form
The CNA Shower Sheets form plays a crucial role in documenting skin assessments during resident showers. However, several other documents often accompany it to ensure comprehensive care and proper communication among staff. Below are six key forms that are frequently used alongside the CNA Shower Sheets.
- Skin Assessment Form: This form provides a detailed evaluation of a resident's skin condition. It includes sections for documenting any existing skin issues, previous treatments, and recommendations for care.
- Incident Report: When any unusual occurrences arise during a shower, such as a fall or injury, an incident report is filled out. This document captures the details of the event for review and helps prevent future incidents.
- Trailer Bill of Sale: This essential document is key for transferring ownership of a trailer, including necessary details like buyer and seller information and the sale price, and can be found at Arizona PDFs.
- Care Plan: A care plan outlines the specific needs and goals for each resident. It is regularly updated based on assessments, including those from the CNA Shower Sheets, to ensure personalized care.
- Daily Progress Notes: These notes provide a summary of a resident's condition and any changes observed during the day. They complement the information in the CNA Shower Sheets and help maintain continuity of care.
- Medication Administration Record (MAR): This document tracks all medications administered to the resident. It is vital for ensuring that treatments related to skin conditions are documented and managed effectively.
- Communication Log: A communication log allows staff to share important updates about residents' conditions. This ensures that everyone involved in the resident's care is informed and can respond appropriately.
These documents collectively enhance the quality of care provided to residents. They facilitate effective communication among caregivers, ensuring that all aspects of a resident's health are monitored and addressed promptly.
More PDF Forms
Roof Inspection Report Template - This document consolidates an inspector's findings into a legally recognized form.
Bill of Ladding - The Supplement section allows for additional information or amendments to the original Bill of Lading.
When handling the sale of an all-terrain vehicle, it's crucial to have the proper documentation, such as the California ATV Bill of Sale, to ensure everything is above board. This form, which captures the necessary information for the transition of ownership, is essential to protect both the buyer and the seller. For a hassle-free experience, you may want to check out California Templates for a convenient fillable version of the ATV Bill of Sale.
262 Form - This document is a key element in avoiding future disputes over vehicle ownership.
Frequently Asked Questions
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to help Certified Nursing Assistants (CNAs) document the skin condition of residents during showers. It allows CNAs to perform a visual assessment and report any abnormalities, ensuring timely communication with the charge nurse and Director of Nursing (DON).
What types of skin abnormalities should be reported?
CNAs should look for various skin abnormalities during their assessment. These include:
- Bruising
- Skin tears
- Rashes
- Swelling
- Dryness
- Soft heels
- Lesions
- Decubitus (pressure sores)
- Blisters
- Scratches
- Abnormal color
- Abnormal skin temperature (hot or cold)
- Hardened skin (orange peel texture)
- Other abnormalities as noted
How should abnormalities be documented on the form?
CNAs should use the body chart included on the form to indicate the exact location of any abnormalities. Each abnormality should be described and numbered for clarity. This helps in tracking changes over time and ensuring proper care.
What should a CNA do if they notice an abnormality?
If a CNA notices any abnormal skin condition, they must report it to the charge nurse immediately. It is important to communicate these findings quickly to ensure the resident receives appropriate care. The charge nurse will then assess the situation and take necessary actions.
Is there a section for toenail care on the form?
Yes, the form includes a section that asks whether the resident needs their toenails cut. The CNA can mark 'Yes' or 'No' based on their assessment. This ensures that all aspects of the resident’s care are considered during the shower.
What happens after the charge nurse reviews the form?
After the charge nurse reviews the form, they will document their assessment and any interventions needed. If further action is required, the charge nurse will forward the information to the Director of Nursing (DON) for additional review.
Where can I find this form?
The CNA Shower Sheets form is available online at www.primaris.org. It is important to use the most current version of the form to ensure compliance with guidelines and standards.